By MATTHIAS OHLDORF | There are strong efforts on the part of the pharmaceutical industry (Moderna) to switch the entire vaccine production to RNA technology, as it can generate astronomical profits. Currently, there is a de facto field trial with Sars-Cov-2 mRNA vaccines by Pfizer BioNTech and Moderna on millions of people. This makes it all the more important to look at what long-term consequences this new technology method can probably have for the human genome, the next generations and thus for the human species.
To explain this question in more detail, we first need to take a closer look at the functional basics of this novel mRNA vaccine technology.
How do the Pfizer and Moderna vaccines work?
Both vaccines (Moderna, Pfizer) are based on mRNA that codes for the so-called spike protein, an envelope protein of Sars-Cov-2. The first two doses are administered 3-4 weeks apart, into the (arm) muscle. Booster vaccines are to be administered annually. Both vaccines are deep-frozen, Pfizer at -70°C, Moderna at – 20°C, to protect the sensitive single-stranded mRNA from enzymatic digestion.
In contrast, the vaccines of the competing products from Astrazeneca and Johnson & Johnson are based on so-called double-stranded vector DNA. The vector, i.e. the transport container into the cell, is in this case a cold or cold virus (adenovirus) that has been genetically modified so that it is unable to reproduce independently in the cell. The vectors of both vaccines are grown on tumourised embryonic stem cells. For Astrazeneca these are embryonic kidney cells (HEK-293) and for Johnson & Johnson these are foetal retinal cells. Apart from ethical questions, the cell lines are based on aborted foetuses, the question of contamination with human DNA is a safety risk, especially since tumour genes can also enter the human organism in this way.
To be protected from enzymes, the strands of the mRNA vaccines are surrounded by an artificial fat or lipid shell. These are lipid nanoparticles (LNP). In addition, the mRNAs are stabilised by modified nucleotides. In this specific case, instead of the naturally occurring nucleotide uridine, this is a variant of uridine that is specially characterised by a so-called methylation: methyl uridine. The mRNA vaccines deliver the spike protein to antigen-presenting cells, activating the immune system [link]. Are the two vaccines really as mature as the manufacturers claim?
Speed first: vaccine development and approval
In the USA and Europe, politicians and authorities thought they had to push the pace on behalf of the pharmaceutical industry: Pfizer’s vaccine was approved for the European market under the brand name Comirnaty by the European Medicines Agency (EMA) on 22 December 2020 after a processing period of only three weeks. A few days earlier, this had been done by the FDA for the US market [link]. In the US, the production and distribution was raised by the manufacturers together with the Defence and Health Departments under the name “Operation Warp Speed”. Proudly, Pfizer announced in a release:
“Today’s conditional marketing authorisation by the European Commission is a historic achievement. It is the first vaccine to be tested and approved in less than a year in a large-scale study in more than 44,000 subjects. This great achievement is based on decades of work by many scientists around the world and is also a confirmation of our successful collaboration with our partner Pfizer,” said Ugur Sahin, M.D., CEO and co-founder of BioNTech. “As a company founded and headquartered in the heart of Europe, we are particularly excited to make our vaccine available to the European population in the coming days. We will be collecting further efficacy and safety data in our study participants over the next two years, as well as evaluating the vaccine against any emerging mutations.”
The same pattern is repeated with the so far wisely omitted approval for infants between 6 months and 5 years: Pfizer received emergency approval for the US market on 17 June [link]. It is only a matter of time before this also happens in the EU. How do approvals normally work and what chances do the different vaccine categories have of getting into patients’ bodies at all?
Vaccine development: simple, complex and unprecedented
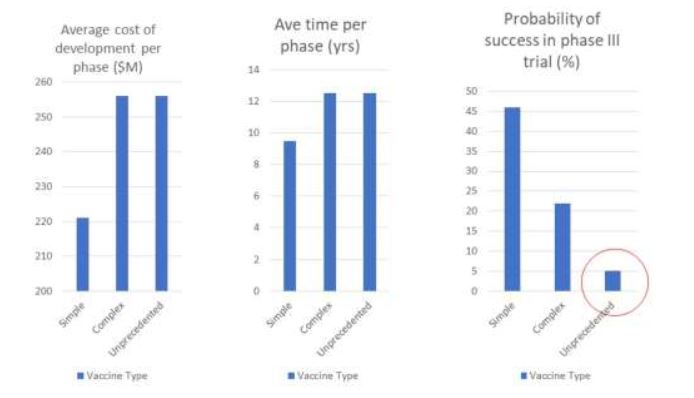
According to a study funded by the Bill & Melinda Gates Foundation [link], there are three categories of vaccines in the approval process: simple, complex and unprecedented. The following illustration provides an overview: The first two categories are standard (simple) or modified (complex) vaccines produced with established technologies. Unprecedented vaccines are those newly developed against diseases for which there has never been a vaccine before, such as HIV or malaria.
Young et al. 2018
Both complex and unprecedented vaccines are extremely costly to approve, with each phase costing around US$250 million and taking an average of 12.5 years. More importantly, the unprecedented vaccine trials have only a 5% chance of even successfully completing Phase II, and even if they clear that hurdle, only a 40% chance of successfully completing Phase III and getting marketing approval. So there is a “low probability of success, especially for unprecedented vaccines” [link].
In addition to the extremely accelerated development time (!) and successful completion of Phase III, two vaccines were also approved almost simultaneously, the one from Moderna [Link] and the one from Pfizer [Link]! In addition, the vaccines from Astrazeneca and Johnson & Johnson, which are based on other mechanisms, also received emergency approvals after a short development period. In view of the above probabilities, coincidences can be ruled out here; it is probably a matter of mafia-corruptive processes. The claimed drug efficacy of 90-95 % (Pfizer) or 94.1 % (Moderna) was called into question early on [Link].
Were foreseeable consequences ignored due to political pressure during the approval process? Is there a danger that the human genome and the genetic material of future generations will be permanently damaged?
Permanent changes in the human genome
The classical linear model of protein biosynthesis, which postulates a one-way street from DNA to mRNA and finally protein translation, has been outdated for decades.
Wikimedia: ADN_planeta_tierra
The enzyme reverse transcriptase, which converts mRNA into DNA, has been known for a long time; initially it was only known from retroviruses, to which Sars-Cov-2 also belongs. For some time now, the enzyme has also been known from so-called mobile DNA elements in the human genome. These make up about 1/3 of the genome! They consist of two elements that belong to the retrotransosons, so-called SINE’s and LINE’s (short and long incoporated nuclear elements). They used to be regarded as functionless “junk DNA”, a view that has since been revised. LINEs convert RNA into DNA using reverse transcriptase, they incorporate RNA from external sources (e.g. retroviruses) into the genome. SINEs rearrange this DNA in the genome, especially in adenosine-thymine rich regions. This results in sometimes extensive genetic changes in the genome.
In addition, the human genome has endogenous retroviruses (HERVs) that closely resemble retroviruses and retrotransposons. A prominent example of such a sequence is the protein syncytin. It allows the fertilised egg (embryo) to implant in the uterine wall and bears a strong resemblance to the spike protein of Sars-Cov-2! There are (controversial) speculations that the activation of the immune system by the spike proteins (as a side effect?) attacks the homologous syncytin and thus makes implantation of the embryo impossible and thus leads to infertility [Link]. There are also exogenous, i.e. infectious and independent retroviruses, which can, however, integrate into the genome.
Confirmed in the lab
Is this a purely academic possibility? Definitely not! A research group has already confirmed the possibility of integrating spike mRNA into the human genome, albeit initially only in cell cultures. The research group came up with this experimental arrangement because they noticed that vaccinated patients repeatedly suffered from Sars-Cov-2 outbreaks [Link]. The long-term consequences of the integration of mRNA into the genome for genetic health cannot be estimated at all! Particularly dangerous: LINE-1 is also active in the gametes, i.e. sperm and egg cells, and thus theoretically enables the incorporation and transmission of foreign RNA to the next generation [Link]. According to a Swedish study [Link], spike protein interferes with the cell’s own DNA repair mechanisms, thus additionally leading to more genome mutations.
What long-term side effects can vaccinated people possibly expect after many years?
Wrongly “folded” proteins: Alzheimer’s and Parkinson’s disease
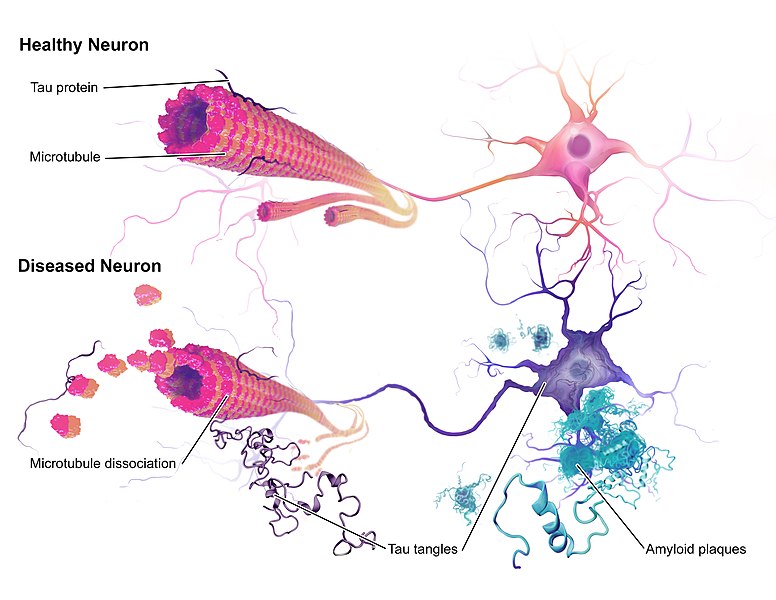
A potential danger for the nervous system comes from the (possibly) infectious spike proteins. Such diseases often only appear after many years or decades. The functionally most important component of both vaccines are Sars-Cov2 spike protein-encoding mRNA molecules, the proteins resulting from protein biosynthesis can form so-called prions. Prions cause degenerative changes in nerve tissue. Known diseases that can be traced back to them are Parkinson’s and Alzheimer’s diseases. Prions are protein molecules that do not exist in their “normal” three-dimensional form (conformation) but are misfolded. They spread by also triggering pathological, i.e. disease-causing, structural changes in neighbouring proteins.
Wikimedia: 776px-Alzheimers_Disease
Over time, prions form fibre bundles and plaques in the nerve tissue. The disease pattern is illustrated by BSE or mad cow disease: the diseased animals, usually sheep or cattle, were fed animal meal from conspecifics suffering from similar diseases damaging the nervous system (TSE and trotter). The ingestion of infectious proteins via the feed (meat-and-bone meal from nerve tissue) triggered the above-described transformation of proteins into prions in the brain. A comparable disease, kuru, caused by ritual cannibalism (ancestor worship) of tribes in Papua New Guinea, also existed in humans until the 20th century.
Spike proteins are transmembrane proteins that protrude through the lipid membranes of cells and have the small amino acid glycine incorporated at both their ends (intracellular and extracellular). This so-called amino acid motif has a high potential to fold over and form so-called ß-sheets, the prion motif. It is abbreviated GxxxG, where “G” stands for the amino acid glycine and “x” for any other amino acid. The artificially produced spike mRNAs, however, have not only one such GxxxG motif, but five! This is a special feature of Sars-Cov-2 that does not occur in other coronaviruses. There is therefore a high probability that prions are formed, with all conceivable pathological consequences for the vaccinated! In addition, the vaccine mRNAs have two built-in changes (amino acid proline), which indirectly also increase the potential for prion formation. Do the mRNA vaccines or the spike proteins produced actually trigger Parkinson’s and Alzheimer’s or comparable diseases? Clinical evidence is (still) lacking, but this is very possible [link, link].
We have described a small selection of the theoretically expected side effects and explanations for the mechanisms behind them and tried to present their occurrence in a generally comprehensible way. There are many more potential and clinically manifest diseases that could be triggered by different components of the two mRNA vaccines from Moderna and Pfizer [link].